Hello, this is Dr. Cha-Young Kang, Director of Nose Lab Clinic. Today, I’d like to discuss a case of septal reconstruction for a contracted nose, an approach we frequently use to address significant nasal deformities and columella retraction.
In contracted noses, severe columella retraction is often present, a common complication resulting from extensive damage to the septal cartilage. When the septum is compromised, the columella may collapse inward, and patients often experience nasal obstruction as well.
This particular patient developed a contracted nose following severe inflammation. At the time of her visit, she had previously undergone complete removal of inflamed tissue, and we initiated a rigorous course of stem cell treatments to expedite healing. After about two months, with inflammation under control, we proceeded with reconstructive surgery using autologous rib cartilage.
During the pre-surgical consultation, we analyzed her nasal structure and noted several key issues:

Her nasal tip was drooping, and the columella was almost invisible in the profile view.
From an oblique angle, her nose appeared flattened, lacking structure and definition, with visible columella retraction.
From the front, her nasal bridge was wide, and the nose appeared slightly crooked, with the alar base drooping due to columella retraction.
The nostrils displayed retraction from previous open rhinoplasty scars, and the columella showed significant retraction.

Surgical Plan
Before proceeding, we completed a full course of stem cell therapy to eliminate any residual inflammation, which consisted of four treatments over two weeks. With inflammation stabilized, we developed a surgical plan to correct the columella retraction and restore nasal structure:
Complete removal of existing filler and silicone implants
Reuse of remaining autologous tissues (rib, septal, and ear cartilage) from previous surgeries
Additional autologous rib cartilage harvest to use as primary graft material
Septal extension graft to refine the nasal tip
New silicone implant at a lower bridge position if no intraoperative inflammation was observed
Given the patient’s right-side nasal obstruction, we performed an examination that confirmed rightward septal deviation. Her CT scans revealed a deviation in the bony section of the septum, significantly narrowing her right nasal airway. With this in mind, we planned a concurrent septoplasty during her septal reconstruction.
Surgery and Findings
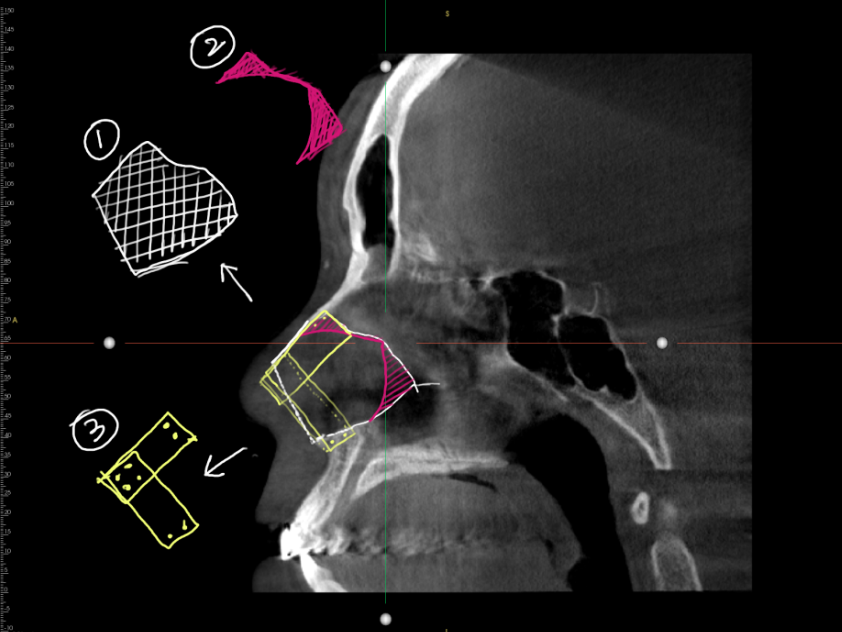
During surgery, we found the septal cartilage was even more damaged than anticipated, with only about 30% of it remaining intact. The remaining septal cartilage (marked as ② in images) was insufficient to support the nasal structure, requiring us to drill into the nasal bones and reconstruct the septum using autologous rib cartilage (marked as ③ in images). We corrected the deviation and removed the septal spur on the right side to improve nasal airflow.
To elevate the drooping nasal tip, we used an additional rib graft as a septal extension and reconstructed the nasal alar cartilage, which had been removed in a previous surgery. To address the appearance of retracted nostrils, we also performed nostril extension surgery.
Since the contracted skin around her nasal tip was significantly tight, we harvested skin and dermis from behind her ear to graft onto both sides of the columella. This approach effectively provided the extra tissue necessary for a seamless closure

Before Surgery (Left) / Immediately After Surgery (Right)

Before Surgery (Left) / Immediately After Surgery (Right)

Before Surgery (Left) / Immediately After Surgery (Right)

Before Surgery (Left) / Immediately After Surgery (Right)
Post-Surgical Outcomes
Post-operative results showed a naturally positioned columella with a nasolabial angle corrected to approximately 95 degrees, enhancing her profile and subtly improving her protrusive lip appearance. From an oblique angle, the starting point of her nasal bridge was lowered, and the nasal tip, once flattened, now had a refined projection. The bridge looked narrower, and the columella retraction was visibly improved, providing a lift to the previously drooping alar base. Nostrils that previously appeared collapsed due to scarring had regained a more natural, symmetrical appearance.
Final Thoughts
Septal reconstruction is a highly complex procedure but is essential for correcting severe septal damage in contracted noses. Following rhinoplasty, complications like columella retraction are common when the septum is damaged. Adding graft material to the columella alone provides only temporary results, as the underlying septal damage is often the true cause of the retraction. Without addressing this, columella retraction tends to recur. Septal reconstruction, which provides the necessary structural support, is often required, and this is a challenging procedure best suited for otolaryngology specialists.
Today, we explored a case where we used autologous rib cartilage for septal reconstruction to correct severe columella retraction caused by inflammation-induced contraction after previous rhinoplasty. I hope this case provides insight for those experiencing similar issues with contracted noses and retracted columella.
Thank you,
Dr. Cha-Young Kang, Director of Nose Lab Clinic.


Commentaires